
Fetal hydrothorax is an accumulation of fluid (effusion) in one or both chest cavities of an unborn child – in most cases, a build-up of yellowish-clear lymph fluid (primary chylothorax), which disappears again within days to weeks after birth. Severe and usually untreatable metabolic disorders or genetic defects are rarely the cause. In such cases, the prognosis remains very poor even after successful prenatal therapy.
If your baby is affected by bilateral hydrothorax, both lungs are prevented from developing due to the ever-increasing amount of fluid. This can lead to severe underdevelopment of both lungs (lung hypoplasia). However, because the pressure of the fluid accumulation often significantly impairs the infant’s heart function and placental blood flow, untreated bilateral hydrothorax is often fatal for the affected child even in the womb.
If the hydrothorax is only on one side, close monitoring is required and it is best to wait and see. However, prenatal surgery may be necessary if the effusion increases rapidly or is already very large and is affecting the heart.
At the DZFT, we have been offering a new minimally invasive procedure since May 2014, which allows large effusions in both halves of your unborn child’s chest to be permanently removed through a single small incision instead of the usual two separate punctures. In addition, much longer shunts are used to minimize the risk of amniotic fluid entering the child’s chest from outside and triggering inflammation.
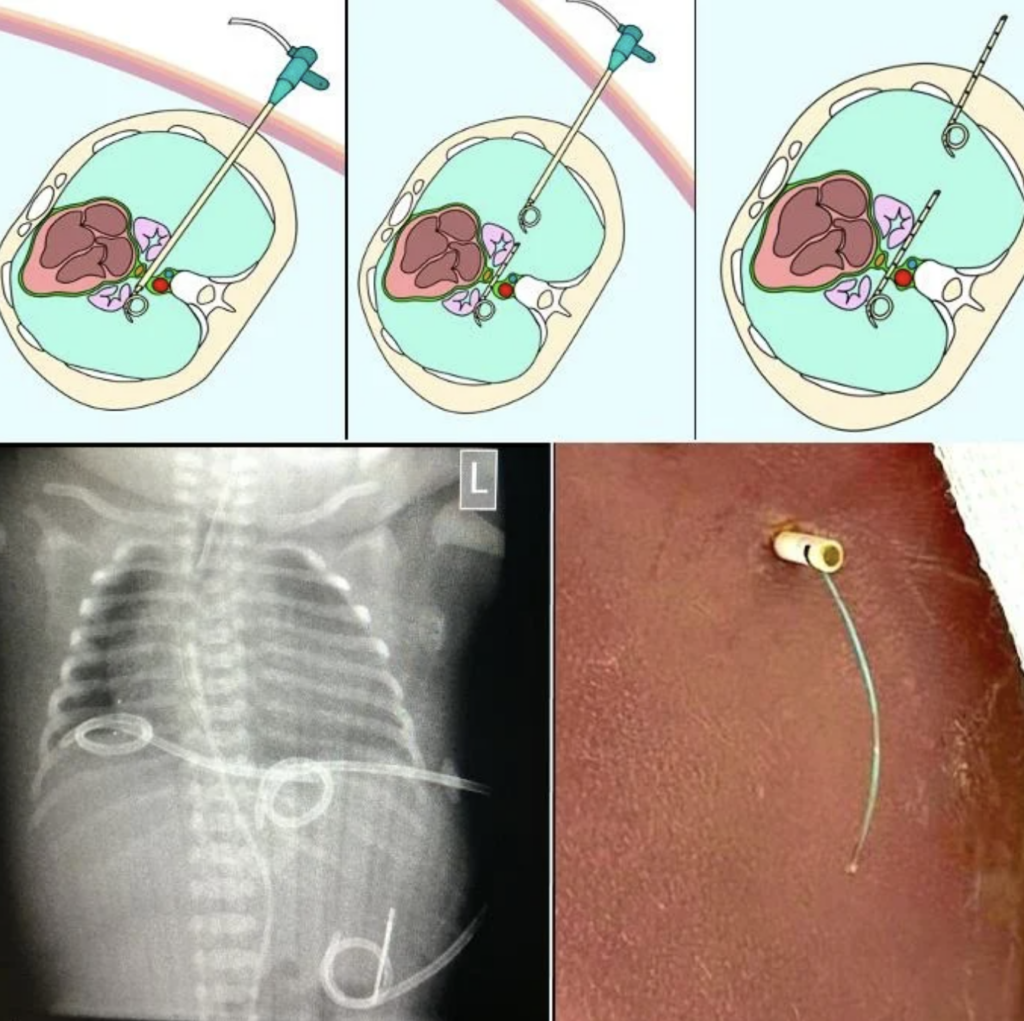

This much less traumatic procedure significantly reduces the risk of premature rupture of the membranes. The administration of sedatives and painkillers makes the procedure safer and painless for both mother and child.
This allows your child’s heart function to return to normal within a very short time. In less severe cases, the lungs expand again immediately and continue to grow, so that your child can be treated effectively after birth.
In some unborn babies, the lungs do not develop sufficiently despite drainage and remain small and poorly supplied with blood. This usually affects children with Down syndrome, Turner syndrome, or Noonan syndrome. In these cases, the windpipe can be closed with a small balloon (FETO) after the shunt has been inserted. This allows their lungs to catch up significantly and improves blood flow. Both advantages optimize the postnatal treatment options for these children.
As a general rule, pregnant women whose child is affected by hydrothorax should immediately go to a gynecological clinic if they experience increasing pressure in the abdomen and pulling pains in the lower abdomen: This condition often leads to a significant increase in the amount of amniotic fluid, which sometimes needs to be drained during pregnancy to prevent premature labor, rupture of the membranes, dilation of the cervix, and premature birth.
Water retention in the tissues and body cavities of the pregnant woman herself can also occur (“mirror syndrome”). This is characterized by sudden significant weight gain and increasing water retention (edema) in both lower legs, as well as shortness of breath. This is an emergency and you should seek obstetric care immediately.
Mirror syndrome can improve after fetal therapy. However, premature delivery is indicated in cases of severe maternal symptoms. Other diseases with similar symptoms must also be ruled out.
Patient comfort and safety are our top priorities
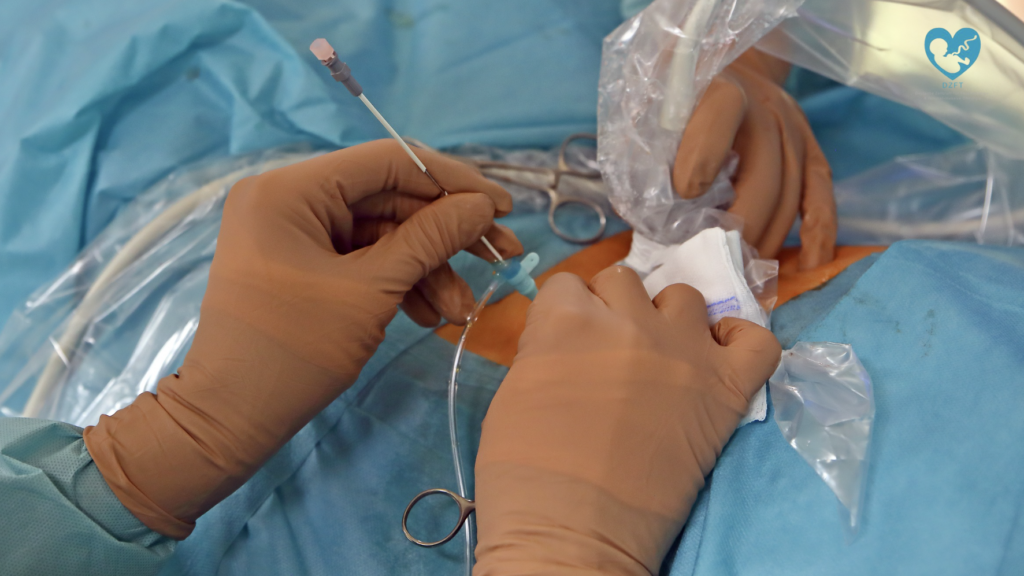
All prenatal shunt procedures in unborn babies with hydrothorax are performed at the DZFT between the 18th and 32nd week of pregnancy in an operating room under short anesthesia with antibiotic prophylaxis.
Thanks to these measures, the technical success rate at our center is well over 90%, even under very difficult conditions. No procedure-related infections have been observed. In addition, bladder rupture, fetal complications, and infections are less common. The stress caused by the procedure for both mother and child is also reduced to a minimum. This is an indispensable advantage, especially in the case of repeated procedures.
As unbelievable as it may sound, pain management for mothers and babies and infection prevention through procedures performed in a dedicated operating room with antibiotics are still not standard practice for prenatal procedures in Germany! We strongly recommend that you take these factors into account when choosing your treatment center!
If you have any further questions about minimally invasive diagnostics and treatment of fetal hydrothorax or would like to obtain a second opinion, please contact the DZFT daily between 10 a.m. and 5 p.m. on 0175/597-1213 or send us an email. If you only reach the answering machine, please leave your name and a telephone number where we can call you back.
If you have already decided to have a procedure performed at another clinic, we will be happy to advise you in this case as well and offer a prognostic second opinion on your child’s condition and treatment.
Please note: The content of our website is for informational purposes only and is not intended to replace personal consultations with us or other recognized medical specialists in this field. For all individual questions and decisions concerning your health and that of your child, we strongly recommend that you and your family members contact us, your doctor, and/or other experts in person.